|
of a 2-Part "Tricks of the Trade" Column |
 |
 |
Thom Dick, EMT-P |
Use of Restraints, PART 1 December 2002 • Volume 27 • Number 12 |
|
Use of Restraints, PART 2 January 2003 • Volume 28 • Number 1 |

I really hate writing a "negative" review of stuff written by folkz I know! And, it doesn't "help" that Thom Dick and I are only "somewhat acquainted." We met somewhere ... sometime (likely at a JEMS EMS Today conference, years ago) – certainly, we've "heard of" each other down through the years. And, I'm reasonably confident that Thom Dick is a caring, and responsible, EMS provider and educator. But, when I read Part 2 of his JEMS "Tricks of the Trade" column about restraints, and saw the pix that accompany it, I was ... AGHAST!!!
"aghast: adj. struck with overwhelming shock or amazement;
filled with sudden fright or horror"
Still, I'll start my review by identifying some POSITIVE aspects of Thom's Restraint Tricks columns. After a strongly positive beginning, I'll segue into identification of the many NEGATIVE aspects of Thom's Restraint Tricks columns.
EXCERPTS from Thom's column are in dark blue text.
Review of "Tie-Downs"
If you've never had a thorough class on how to restrain someone, you need – and deserve – one. Do yourself and your whole agency a favor: Ask for one today. And if it hasn't happened a month from now, insist on it – and insist on it again – until you become the EMT from hell. (EMTs from hell get things changed.)
Right ON, Thom!
3. When somebody calls 9-1-1, either they can describe their emergency (SOB, chest pain, stabbing, etc.) or they are clearly impaired. When you respond, you deserve to know what you're responding for. Insist on that much from your dispatchers, or ask for the PD to respond and evaluate the situation prior to your arrival.
Right ON, Thom!
4. Take a critical look at every scene before you go waltzing in like a dumb***. Things are supposed to make sense. If they don't, they're dangerous until proven otherwise.
I wish Thom had expanded upon this point, just a bit: If, after a "critical look," the scene still doesn't "make sense" ... doesn't seem "right" to you ... DON'T GO IN!!! Summon law enforcement and wait at a safe distance, until you are ASSURED that it is SAFE for you to go "waltzing in." There is no way in **** that you can help ANYone if YOU become a patient!
5. Don't run, no matter what you see and no matter how frantic people seem to be when you arrive. Walking gives you more time to analyze what's going on and keeps your catecholamines under control so you can think and communicate more clearly. (It also prevents the jitters.)
Right ON, Thom!
8. Most violent situations in EMS result from our own disrespect. Remember your role as a caregiver, and treat patients and their families with dignity and respect – even if they're cranky (on what may be the worst day of their lives).
I wholeheartedly agree that responder "disrespect" (something that happens because we get impatient, or because we harbor prejudices against certain patients) often results in "violent situations." I wholeheartedly agree that treating ALL patients with respect will significantly minimize the likelihood of responder-escalated "violent situations."
Use of Restraints, PART 1
Be a "squeaky wheel!" Yeah, it's a "risk." But, if YOU don't do it, who will? And, if no one does it, NO ONE will get the training they "need – and deserve!"
Since money is often an issue when it comes to getting the best possible training, pool your resources. Encourage your service's Education Officer to contact the individuals who organize your State (or Regional) EMS Conference. Request that they visit my Web Site, and hire me to provide restraint training at your conference(s).
In the mean time: USE MY WEB SITE! Learn all you can from my "All Tied Up And No Place To Go" and "Restraint Asphyxia – Silent Killer" articles. Encourage your coworkers to learn from my web site! Empower yourself and your coworkers by becoming educated, safe and effective, restraint providers.
I'll be quoting Thom in April, 2003, when I address an EMS Dispatchers conference. Dispatchers are the "first link" in any emergency response. Well-educated dispatchers certainly would KNOW to pass along information about the calling party speaking as though they had an "altered level of consciousness." But, if we don't educate Dispatchers as to what information is important to responding providers, they won't know to pass it along. Consequently, even though they don't "perform" patient restraint, Dispatchers need to – at least – be educated as to the WHYs of patient restraint. In that way, they'll be much better able to identify calls with a potential need for restraint ... much more likely to pass that information along!
Just being dispatched to an emergency stimulates "Fight/Flight" system adrenalin ("catecholamine") release. Running stimulates an even greater adrenalin release! Adrenalin-tweaked responders are impatient and make poor decisions (like entering scenes they shouldn't). Adrenalin-tweaked responders incompletely assess patients ("miss" vital clues, signs and symptoms) ... misdiagnose injuries and illnesses ... and – because of all that stuff – provide inadequate treatment. The only time you should ever run, is when you're in danger. Then, RUN AWAY ... drop all equipment and GET OUT!!!
(Worrying about being considered a "whimp" can kill you. Just GET OUT!!!)
(Here comes the "BUT..."!)
BUT! "Violent situations" are the LEAST-often-encountered reasons for restraining an emergency patient! Plz see the "REASONS For EMERGENCY PATIENT RESTRAINT" section of the INTRODUCTION to my (currently under construction) DEFINITIVE PATIENT RESTRAINT PROTOCOLS.
And, by focusing only upon "violent situations" when addressing "restraint," Thom is promoting the continued MISINTERPRETATION of the REASONS for patient restraint. Misinterpretation of patient restraint reasons promotes INAPPROPRIATE (and dangerous!) restraint performances.
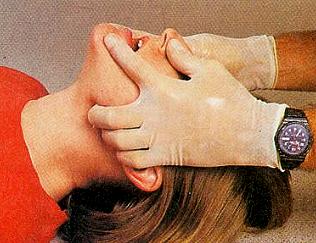
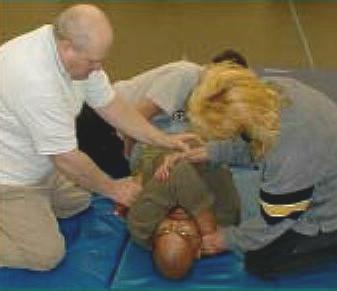
For example; In Part 2 of his Restraint Tricks of the Trade column, Thom Dick promotes INCREDIBLY DANGEROUS RESTRAINT TECHNIQUES ... techniques inconsistent with patient "care" provision ... techniques that even interfere with patient care provision.
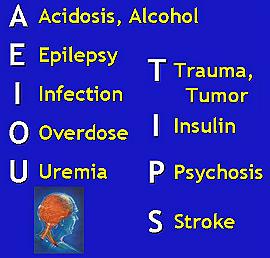
I don't want to believe that Thom did this "on purpose." I want to believe that he did it only because he's never been adequately educated about restraints. I want to assume that Thom has simply forgotten the fact that MANY causes of an altered level of consciousness are productive of violent behavior, and require MEDICAL ASSESSMENT AND TREATMENT.
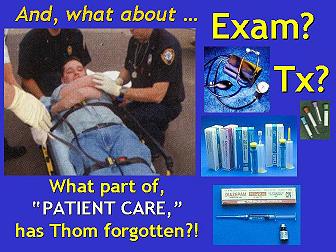
Unfortunately, all providers who follow the directives offered in Part 2 of Dick's Restraint Tricks, will be entirely unable to provide definitive MEDICAL ASSESSMENT AND TREATMENT to the individuals they restrain – no matter WHAT caused their altered level of consciousness.
 |
|
"Use of Restraints, Part 2" column. EXPLAINED THOSE THINGS in my "All Tied Up And No Place To Go" and "Restraint Asphyxia – Silent Killer" articles. |
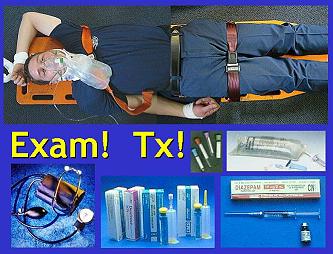
Essentially, most of Thom's "Use of Restraints, Part 1" column is helpful. But, the ONLY helpful aspect of "Use of Restraints, Part 2" is Thom's provision of photography that clearly demonstrates examples of WHAT NOT TO DO when restraining patients!
After calling his attention to the information provided by my review, Thom Dick (and JEMS) refused to publish a "RETRACTION" of any information contained in his "Use of Restraints, Part 2" column. I'm not surpriZed. Obviously, it is painfully difficult to admit when you are WRONG – even when you are clearly demonstrated to be WRONG.
Consequently, in order to bring the reasons for why Dick's "Use of Restraints, Part 2" column should NOT be followed to public attention, OTHERS have to write to JEMS, providing their opinions of Dick's "Use of Restraints, Part 2" column, so that.
I strongly encourage EVERYONE to write their OWN review
FAX: 619 - 699 - 6246
Email JEMS Editor:
of Thom Dick's / JEMS' "Use of Restraints, Part 2" column.
Send your review to JEMS, as a "Letter To The Editor."
JEMS Letters
525 B Street, Suite 1900
San Diego, CA 92101-4495
 jems.editor@elsevier.com
jems.editor@elsevier.com
THEN, SEND ME a copy of YOUR LETTER TO JEMS' EDITOR!
c-d-miller@neb.rr.com
REFERENCES:
Weiss EM, et al.; Deadly restraint. A Hartford Courant investigative report. http://www.copaa.com/newstand/day1.html October 11, 1998.
Claudio Cruz and Felicita Cruz, Administrators of the Estate of Claudio Cruz, Jr., vs. Allegheny Valley School, et al; in the Court of Common Pleas, Philadelphia County; CAUSE NO. 002361.
Miller, CD; "Restraint Asphyxia – Silent Killer" http://www.charlydmiller.com/RA/restrasphyx01.html.
Email Charly at: c-d-miller@neb.rr.com