
 |
 |
of Frequently Misinterpreted and Misrepresented Restraint Research PART THREE |
CITATION:
Miller CD. A comprehensive review of frequently misinterpreted and
misrepresented restraint research; Part three. April, 2005.
http://www.charlydmiller.com/LIB05/2005chasresearchreviewpart3.html
 NEW as of December, 2005:
NEW as of December, 2005:
A 39-page PDF FILE containing All 3 Parts & the References!
If you’re going to PRINT any part of this 3-part Comprehensive Review, print from the PDF file. The webpages end up printing weird (text next to photos bumps the photos to another page). Plus, printing all these parts and the reference list from the webpages takes up a lot more than 39 pages.

NEW as of January, 2006:
Eisele JW, Chan TC, Vilke GM, Clausen J.
Comparison of Respiratory Function in the
Prone Maximal Restraint Position With and Without
Additional Weight Force on the Back
The unpublished paper presented at the annual meeting of the
American Academy of Forensic Science, in Reno, Nevada: February 21-26, 2000.
Chan TC, Clausen J, Neuman T, Eisele JW, Vilke GM.
Does Weight Force During Physical Restraint
Cause Respiratory Compromise?
Ann Emerg Med, October 2003;42(4),
The unpublished paper presented at the 2003 ACEP meeting, and posted in the
ACEP Research Forum Supplement: pS17.
Chan TC; Neuman T; Clausen J; Eisele J; Vilke GM.
Weight Force During Prone Restraint and Respiratory Function
Am J Forensic Med Pathol 25(3):185-189, September 2004.
CHAN’s published report of the 1999 study previously represented by
paper presentations at two other medical professional society’s meetings.
Vilke GM, Michalewicz B, Kolkhorst FW, Neuman T, Chan TC;
Does Weight Force During Physical Restraint
Cause Respiratory Compromise?
Acad Emerg Med May 2005;12(5 Supplement 1): page 16.
The unpublished paper presented at the May, 2005, Annual Meeting of the
Society for Academic Emergency Medicine.
The COMPREHENSIVE REVIEW of ARTICLE # "3":
Chan TC; Neuman T; Clausen J; Eisele J; Vilke GM.
Weight force during prone restraint and respiratory function.
Am J Forensic Med Pathol, September 2004;25(3):185-189.

RELATED BACKGROUND INFORMATION:
This study and its published report has a very … interesting … history.
This article is the THIRD incarnation of the study’s report,
and is the only version that has ever been published as a journal article.
A paper-presentation of this study’s findings was FIRST presented at the annual meeting of
the American Academy of Forensic Science, in Reno, Nevada; February 21-26, 2000:
Eisele JW, Chan TC, Vilke GM, Clausen J:
Comparison of Respiratory Function in the Prone Maximal Restraint Position
With and Without Additional Weight Force on the Back
This means that the actual “Weight Force” STUDY had to have been performed prior to February, 2000. Likely, the study was performed some time in 1999 – more than 4 years before Chan finally found someone to “publish” it!
The original “lead” study author, and the AAFS 2000 conference Presenter, was Dr. Eisele.
RUMOR has it [I’ve honestly forgotten when or from whom I heard this! But, it surely was some time in 2002, and surely from a California physician who knows Dr. Eisele and the Chan et al gang.] … RUMOR has it that Dr. Eisele didn’t feel the study had yielded information that was in any way worth bothering to publish. Consequently, he wasn’t interested in pursuing the study’s publication.
[When I first posted the above rumor (September, 2004), I included the following note: Dr. Eisele! If you wish to “refute” this rumor, PLZ contact me and testify to same in writing! I’ll happily retract the “rumor” if you give me a reason to! I have yet to hear a peep from Dr. Eisele. However, the offer still stands.]
Whether or not Dr. Eisele felt that the study yielded information that was in any way worth bothering to publish, the American Academy of Forensic Science (the conference host) clearly did NOT. Had the AAFS felt that the study’s report was in any way worthy of publishing, the paper would have progressed to become an article in the AAFS’ publication, the Journal of Forensic Sciences.
It did not.
When the study’s information surfaced again – over three years later, as another conference paper presentation – I found it terrifically interesting (especially considering the rumor about Eisele’s opinion of its findings) that CHAN was suddenly cited as the “lead” author and paper Presenter. Additionally, Neuman’s name was added to the “author” list, and Dr. Eisele’s name was bumped back to just before Vilke’s name:
Chan TC, Clausen J, Neuman T, Eisele JW, Vilke GM.
Does weight force during physical restraint
cause respiratory compromise?
Ann Emerg Med, October 2003;42(4), ACEP Research Forum Supplement: pS17.
Chan’s paper presentation paper was a slightly-altered version of Eisele’s 2000 AAFS paper presentation, and was presented by Chan in October of 2003, at the American College of Emergency Physicians conference in Boston.
I’ll identify the significant alterations Chan made in an upcoming section of this review.
What is important to note HERE; had the ACEP peer-reviewers considered Chan’s representation of this study’s findings to be in any way worth bothering to publish, Chan’s paper presentation would have progressed to become an article published in ACEP’s publication, the Annals of Emergency Medicine.
It did not.
Consequently, not only is the Am J Forensic Med Pathol September 2004, “Weight force during prone restraint and respiratory function” article the THIRD-version report of a study that was performed prior to February of 2000, it took Chan more than four years to find someone willing to bother publishing it.
Additionally, within his 2004 version of its report, Chan entirely failed to identify the DATE that the study was performed. Thus, only the few people who attended the 2000 AAFS and/or 2003 ACEP conferences – or the very few people who carefully monitor Chan’s track record for misinterpretation and misrepresentation – could possibly have known that Chan’s report is that of study information obtained back in 1999.
EVIDENCE of CHAN’S MISREPRESENTATION &/or
MANIPULATION of the STUDY’S INFORMATION:
Chan’s misrepresentation and manipulation of the study’s information is most clearly demonstrated by his descriptions of how the study subjects were selected for, or excluded from, study participation.
From Eisele’s 2000 AAFS paper presentation:
“Ten healthy volunteers were recruited and informed of the procedure, and gave verbal and written consent. They were screened for pulmonary function in the sitting position and rejected if baseline forced vital capacity (FVC) or forced expiratory volume in one second (FEV1) were outside of acceptable limits.More than three years later, in his 2003 ACEP paper presentation, Chan stripped this study subject selection description down to the following:
…
Although body size and habitus are matters of concern in evaluating the effects of restraint, the subjects in this study were intentionally kept within an average range;” [range undefined]
“Ten volunteers completed a randomized crossover, controlled trial in a pulmonary function laboratory.”More than four years after the study was performed, here is the study subject selection description that Chan managed to have published:[That’s it! That is the ENTIRE study subject selection description offered by Chan in his 2003 ACEP presentation paper!]
“We performed a randomized, cross-over, controlled trial on 10 subjects placed in 4 positions for 5 minutes each …”“Ten volunteer male subjects between the ages of 18 and 45 years were recruited to participate in the study. Potential subjects were excluded if they were unable to be placed in PMRP. No exclusion was made on the basis of pulmonary or cardiovascular disease or function, or based on body size and weight.”
… “Subjects ranged in age from 21 to 40 years, and body mass index ranged from 21.3 to 35.3 kg/m2. There were no exclusions of any participant or subject data.”
Considering the above facts, here are the CONCLUSIONS that can legitimately be drawn regarding Chan’s REPRESENTATION of the 1999 “Weight Force” study’s subject exclusion descriptions, and the questions prompted by same:
What possible reason could Chan have for leaving this terrifically significant factor OUT of his 2004 study report? Is it – perhaps – that Chan is motivated to “down-play” the fact that all the study subjects were perfectly HEALTHY individuals?
Does it mean that some study subject candidates were excluded merely because they felt uncomfortable when placed in the PMRP position?If a study subject candidate’s “inability” to be placed in a prone and pseudo-hogtied position was not related to his body size and weight – if it was not related to his simple complaint of discomfort when placed in the study position before weight addition – then, WHAT was the genesis of this exclusionary “inability”? And, again, WHY didn’t Chan bother to explain this when he was finally given the opportunity to publish the study’s report?
Yet, in Dr. Eisele’s February 2000 paper presentation, Eisele very clearly stated that “the subjects in this study were intentionally kept within an average range.”So? Who was lying … er … misrepresenting study subject inclusion / exclusion parameters – Eisele or Chan?Considering the fact that Dr. Eisele has never (to my knowledge) been evidenced to have the same BIAS that Chan has historically been evidenced to have [See Part One of this Comprehensive Review], I am entirely confident that CHAN is the person who misrepresented study subject body size and weight considerations related to study subject inclusion / exclusion parameters – not Eisele.
Dr. Eisele had absolutely no conceivable motivation to FABRICATE such very specific screening parameters when creating his February 2000 paper presentation of this 1999 study’s information.Thus, within his 2004-published report of this same 1999 study’s information, it is abundantly clear that Theodore Chan point-blank LIED when he reported that “No exclusion was made on the basis of pulmonary or cardiovascular disease or function …”
But, because Eisele’s 2000 paper is so brief, it remains entirely unknown how many OTHER study information misrepresentations (or outright lies) Chan may have perpetrated in his 2004 report. After all, whatever motivated Chan to lie about and misrepresent test study subject exclusion parameters, may also have motivated him to lie about or misrepresent any number of other study finding aspects.Basically, the lies and misrepresentations so clearly demonstrated by Chan’s “version” of the 1999 weight study test study subject exclusion information, entirely destroy any single shred of CREDIBILITY that Chan may have retained prior to this article’s publication. Unfortunately for future victims of forceful-prone-restraint asphyxia, only those who read this review will likely ever learn of Chan’s lack of credibility.
ANOTHER Example of Chan’s Affinity for
Gross Misrepresentation of Information
is Demonstrated by the Following Text
from his 2004-Published Report:
Chan writes:
“Some have argued that the PMRP [Prone Maximal Restraint Position] prevents adequate chest wall, abdominal, and diaphragmatic movement, leading to hypoventilatory respiratory compromise and risk for death from so-called positional asphyxia.12 However, case reports and case series of the sudden deaths of restrained individuals do not clearly indicate a specific mechanism.4–7 Historical as well as autopsy evidence is often unrevealing as to a clear cause of death. Importantly, similar sudden deaths have been reported in patients who were not restraint[sic] in the PMRP, but simply in the prone, supine, lateral side, and even sitting positions.13,14”
Clearly, Chan is dramatically alleging that case reports have been published identifying individuals DYING when simply (without force) being positioned “in the prone, supine, lateral side, and even sitting positions.” Chan even infers that these case reports identifying “simple” – without force – restraint deaths are more “important” than all other published evidence, when considering the legitimacy of case studies identifying deaths being caused by [what Chan styles as] “so-called positional asphyxia”!
WELL. Let’s look at the two references containing the published “case reports” that Chan cites in order to apparently provide SUPPORT his profoundly dramatic allegation – shall we?
Chan’s 2004 Reference “13” is Park KS, Korn CS, Henderson SO.
Agitated delirium and sudden death: two case reports.
Prehosp Emerg Care. 2001;5:214–216.
[MY boldface treatment of text within the following quotes.]

Park/Korn/Henderson Case #1:
Park/Korn/Henderson’s Case #1 did NOT indicate a “simple” supine restraint position. In fact, they didn’t indicate the MANNER in which the patient was supinely restrained – at ALL!
“strapped to the gurney in a supine position.”
In fact, an ambulance wheeled stretcher’s SAFETY BELT |
|
 Standard Safety Harness System |
Furthermore, even after the initial (unknown) manner of forceful supine strapping to the gurney was accomplished, the paramedics still were “unable to obtain vital signs due to the combative nature of the patient.” Thus, one can realistically and reasonably presume that the paramedics employed more and more forceful methods of “strapped” or manual forms of restraint (to more and more unknown portions of the patient’s body) in continued efforts to obtain vital signs. During this activity, the patient entered “cardiopulmonary arrest with an asystolic rhythm.”
[BTW: Those who do not recognize the significance of a patient entering cardiac arrest with an initial ECG of “pulseless electrical activity” or “asystolic rhythm” should review their ACLS texts … specifically refreshing their memory of the most frequently-occurring dysrhythmia following a “simple” or “common cardiac arrest” vs. the most frequently-occurring dysrhythmias following an ASPHYXIAL cause of death.]
BOTTOM LINE: Park/Korn/Henderson’s Case #1
did NOT indicate a death occurring during “simple” supine restraint position.
Park/Korn/Henderson Case #2:
“A 41-year-old African American woman with a history of polysubstance abuse was brought to the ED by police and paramedics for bizarre behavior including slamming her head against a brick wall. On arrival, she was combative, speaking in incoherent sentences, and refusing to stay on a gurney. … The safety personnel placed her in a sitting position on the gurney with her wrists handcuffed to her ankles. The patient suddenly collapsed with no spontaneous respirations or pulse. Cardiopulmonary resuscitation was initiated. Electrocardiographic monitoring revealed pulseless electrical activity, …”
Park/Korn/Henderson’s Case #2 did NOT indicate a “simple” incident of restraint while “even sitting” causing death! In fact, the authors clearly indicated within their report that the victim was NOT in a “simple” seated position when she died.
“Safety personnel had placed the patient in a sitting position with her wrists handcuffed to her ankles, so that she was bent forward, placing pressure on her chest, a risk factor for positional asphyxia.”
 |
|
 |
Still, the above two graphics give you an idea of what aspects of Case #2’s restraint position would have looked like.Simply visualize the victim seated on an ambulance wheeled stretcher. Being on a wheeled stretcher, her knees could not have been flexed much (if at ALL, depending upon how her legs were restrained to the stretcher). So, her legs were probably straight out in front of her body.Thus, handcuffing her wrists to her ankles while seated on an ambulance wheeled stretcher would cause her to be SIGNIFICANTLY bent-over (forward) at the waist, and would seriously interfere with her abdominal excursion – seriously interfere with her diaphragm’s ability to generate adequate breathing efforts.
Granted, Park/Korn/Henderson’s 2001 case discussion’s evaluation of why this victim suffered respiratory interference while restrained in the manner they reported was WRONG.
It wasn’t “pressure on her CHEST” that impeded her mechanical ability to breathe – the structure of her ribcage would have prevented such impedance! It was BELLY MOVEMENT (abdominal excursion) interference caused by her bent-forward “sitting” restraint that interfered with her DIAPHRAGM (the largest and most important respiratory muscle) from functioning so as to generate adequate breathing efforts. Thus (as with forceful-prone-restraint), ABDOMINAL RESTRICTION is what interfered with her mechanical ability to breathe.
But, even given this inaccurate cause of respiratory arrest discussion, Park/Korn/Henderson’s case study #2 CERTAINLY offered no indication that a “simple” incident of restraint while “even sitting” had caused this victim’s death! If Chan actually read this case study, he could not help but know that.
Consequently, it appears that Chan cited a case study that he KNEW did NOT represent an incident of “simple” seated restraint causing death, so as to provide support for a statement he knew to be erroneous!
In other words, Chan lied.
Well, gosh! Perhaps Theodore Chan was merely … MISTAKEN … when citing reference 13 to support his incredibly dramatic statement that case reports have been published identifying individuals DYING when simply (without force) being positioned “in the prone, supine, lateral side, and even sitting positions.”
So, let’s look at the SECOND reference Chan cited in support of his statement:
Chan’s 2004 Reference “14” is Hick JL, Smith SW, Lynch MT.
Metabolic acidosis in restraint-associated cardiac arrest: a case series.
Acad Emerg Med. 1999;6:239–243.
This is a relatively wonderful case report series! It’s one of the first to identify and call attention to the profound acidosis that accompanies restraint asphyxia deaths, vs. the very much LESS acidotic pH that accompanies “simple” or “common” cardiac arrest victims.
And, this case report series discusses 5 different incidents of restraint asphyxia.
[Again, MY boldface treatment of text within the following case report quotes.]
Hick/Smith/Lynch Case #1:
“A 36-year-old man was acting extremely agitated and belligerent on a downtown sidewalk. … attacked a police officer and ran. … subdued by several officers. … transported to the ED, where he continued to fight vigorously while lying prone with his hands cuffed behind him. … Shortly thereafter, the patient had a witnessed respiratory arrest. … Shortly after intubation, a 15-second episode of asystole was noted;”The phrase, “he continued to fight vigorously while lying prone with his hands cuffed behind him” suggests that there was something for him to “fight” against, during his efforts to get out of the prone position. It suggests that manual and/or mechanical forms of restraint were maintaining him in a prone position. That’s not someone “simply” dying while in a prone position.
No help for Chan’s statement here.
Hick/Smith/Lynch Case #2:
“A 39-year-old-man with a history of unspecified psychiatric illness was brought to the emergency psychiatric area for evaluation of agitation and psychosis. The patient became violent and was restrained by several security guards. He was placed prone with his arms behind him. During the restraint process he became apneic and pulseless.”“During the [prone] restraint process” is not an indication of someone dying while “simply” in a prone position. It indicates that forceful-prone-restraint was actively being applied at the time the victim “became apneic and pulseless.”
No help for Chan’s statement here.
Hick/Smith/Lynch Case #3:
“30-year-old man … after a long foot chase was apprehended by two witnesses who sat on the patient to restrain him. He lost consciousness, and when the paramedics arrived, he was in cardiac arrest with an idioventricular rhythm. … pH 6.8 …”This discussion fails to identify whether the two witnesses “sat on the patient” while he was prone or supine. However, it is entirely unlikely that even “lay” individuals (those without a “medical” education) would sit on top of someone’s chest or belly while they were SUPINE. Thus, it is far more likely that the victim was PRONE while being sat upon.
Please also note the extremely acidotic pH and the initial pulseless idioventricular rhythm documented. Those things do NOT accompany “acute” or “common” cardiopulmonary arrest. But, they DO accompany deaths caused by forceful-prone-restraint asphyxia.So, NO HELP for Chan’s statement here.
Hick/Smith/Lynch Case #4:
“After firing a gun in an apartment, a 39-year-old-man was apprehended and restrained by several police officers. He continued to struggle during transport in a prone position with his hands cuffed behind his back. Upon entering the ED, he violently kicked a door, and then had a sudden cardiopulmonary arrest. … presenting rhythm was idioventricular … died.”Since “He continued to struggle during transport in a prone position” he had to have been FORCEFULLY – by manual and/or mechanical means – maintained in the prone position while on the wheeled stretcher. That is not an indication of someone “simply” being in a prone position.
Furthermore, how-in-hell could someone who was prone-restrained to an ambulance wheeled stretcher “violently [kick] a door” while “entering the ED”? That’s physically impossible. Consequently, there CLEARLY (even to non-medically-educated individuals) are several activity descriptions MISSING from this case report!How did he get loose enough to violently kick a door? What manner of restraint was used to “subdue” him after he violently kicked the door? What manner of restraint was being employed at the moment he suffered a so-called “sudden cardiopulmonary arrest”?Oh, surpriZe! After arriving in an exam/treatment room of this ED, his “presenting rhythm was idioventricular” … and his pH was “less than 6.8.” Obviously, both his “presenting rhythm” and his ABG blood draw were obtained after the missing bits of information that RESULTED in his “sudden cardiopulmonary arrest” occurred.This was not a case of someone dying while “simply” restrained in a prone position.STILL no help for Chan’s statement here.
Hick/Smith/Lynch Case #5:
“A 38-year-old-man … The patient was wrestled to the ground, maced, and then carried to the median and placed on his side. He continued to struggle, then had a sudden cardiopulmonary arrest.” … he was chemically “resuscitated” in the emergency department … admitted to ICU … “Refractory hypotension and disseminated intravascular coagulation led to an eventual bradyasystolic arrest ten hours after admission.”Oh, so CLOSE, Ted!
But, there is absolutely nothing in this Hick/Smith/Lynch case scenario suggesting that the patient REMAINED “on his side” after the time that he “continued to struggle.”In fact, after being dumped on the median “on his side,” when the subject resumed his “struggle” it is entirely probable that the police officers resumed their manual restraint application. To do so, it is far more likely that the police officers resumed their manual restraint application by first returning him to a PRONE position. It is entirely unlikely that police officers kept him on his SIDE when resuming their manual restraint of this individual.After all, if this individual had remained on his side while simply struggling against his restraint on the median, or had he remained on his side during the police officers’ resumption of manual restraint, there would be no reason for him to have died. So, again, NO HELP HERE, TED.
SUMMARY of EXAMINATION of the
TWO REFERENCES OFFERED BY CHAN
to SUPPORT his argument that
“similar sudden deaths have been reported in patients who were not restraint[sic] in the PMRP,
but simply in the prone, supine, lateral side, and even sitting positions.”:
Hey! I’m happy to be generous when I can be. So, I’ll agree to give Ted the benefit of a doubt here.
However, this is the last benefit of a doubt that I can offer Chan, no matter how generous my mood.
SUMMARY of the ABOVE TWO POINTS:
Each of his “co-authors” allowed him to do so.
Each of his “co-authors” allowed him to do so.
Were he able to prove me WRONG, Ted likely would launch a civil suit against me for “libel” or “defamation of character” or the like.I have absolutely NO fear of such a suit being successfully brought against me. Because, whereas I can show ample evidence demonstrating that my accusations are true, Chan cannot show ANY evidence supporting a claim that my accusations are false.
The OTHER “PROBLEMS” with Chan’s 2004
“weight force during prone restraint and respiratory function”
report of this 1999 study’s results remain exactly the same
as when its findings were presented by Eisele in 2000.
But, now that Chan has finally managed to get HIS VERSION of the study’s findings published (more than 4 years after the study was performed) – and now that I have at least Chan’s version of its full-report, I have identified SEVERAL MORE erroneous misrepresentations promoted by Chan et al.
Unfortunately, I don’t have the time to identify, discuss, and post them EVERY SINGLE ONE OF THEM at this writing. [One of these days, I’ll get to it! But, don’t hold your breath!]
However, I’m happy to take the time to again identify the most important 4-year-old PROBLEMS with this study – and, I’m happy to discuss at least one additional, terrifically SIGNIFICANT, problem related to this study’s methods that only occurred to me after reading Chan’s 2004 representation of it.
(1) All of the 1999 “weight force during prone restraint and respiratory function” study subjects were entirely HEALTHY individuals of “average” weight range.
All of the 1999 “weight force during prone restraint and respiratory function” study subjects were entirely HEALTHY individuals of “average” weight range.
As previously discussed in Part One of this Comprehensive Review (my review of Chan et al’s November, 1997, “Restraint Position and Positional Asphyxia” article), multiple experts agree that information derived from such a clinically-controlled restraint study of healthy individuals’ responses has absolutely no realistic relationship to the effects that a victim of ANY of the multiple causes of altered level of consciousness (an “unhealthy” individual) might suffer during forceful-prone-restraint application.
HEALTHY individuals resisting arrest do not generate enough strength of combativeness to prompt application of forceful-prone-restraint in the manner (or for the length of time) that has repeatedly resulted in death of individuals who were suffering from an altered level of consciousness productive of prolonged violent and agitated behavior (“excited delirium” victims).
Yet, even when a study of prone-restrained HEALTHY individuals demonstrates “that weight placed on the back during maximal restraint does cause a decrease in spirometry parameters,” Chan et al persist in pooh-poohing this kind of decrement (and others like it).
(2)Chan et al were forced (in order to pass a “peer-review” of their article, and finally get it published)
to ADMIT IN PRINT that:
“Our study has limitations. First, as this was a laboratory physiology study, we could not reproduce all conditions encountered in the field setting with such cases. In particular, we did not simulate trauma, struggle, drug intoxication, and other physiologic and psychologic stresses that commonly occur with individuals who are being restrained in the field setting.”Yet, Chan et al elected to publish a “conclusion” that ENTIRELY NEGLECTED to mention the NEGATIVE findings determined by their study. In fact, Chan et al purposefully published a “conclusion” that semantically down-played the importance of the “negative” information derived from their (albeit inadequately-constructed) study.:AND
”Second, the amount of weights selected for this study may not reproduce the actual amount of weight force used on individuals during the restraint process. It is possible that heavier amounts of weights would have impacted respiratory function to a greater degree. Similar to traumatic or mechanical asphyxia cases, extreme amounts of weights could have resulted in significant chest wall trauma and marked elevations in intrathoracic pressure that could have impacted cardiovascular function.”
“We conducted a study on the impact of weight force placed on the back of individuals in the PMRP on pulmonary and respiratory function. We found that weight force of 25 and 50 lbs did not result in evidence of hypoxia or hypoventilatory respiratory compromise in our study subjects.”Basically, as they did in the two previous articles I’ve comprehensively reviewed, Chan et al elected to present study information CONCLUSIONS in a manner that suggests and infers their study having proven that real-life application of forceful-prone-restraint with “weight force placed on the back” DOESN’T HARM ANYONE!
Given my knowledge of Chan et al’s motivation for BIAS regarding the subject manner of restraint asphyxia, their wording of the “conclusion” they manufactured based upon their inadequately-constructed 1999 “weight force” study comes as NO surpriZe to me. It simply continues to make me angry. And, continues to cost me a ton of time having to explain why seemingly-“professional” medical personnel would so grossly and negligently misrepresent information derived from their studies.[Again, see Part One of this Comprehensive Review (my review of Chan et al’s November, 1997, “Restraint Position and Positional Asphyxia” article).]
(3)The amount of WEIGHT employed for this “Weight Force During Prone Restraint and Respiratory Function” study was ludicrously LIGHT, and it was applied to the study subjects in a LOCATION that was GUARANTEED to effect the LEAST amount of interference in respiratory function!
Way back in 2002, when I first was made aware of Dr. Eisele’s 2000 American Academy of Forensic Science conference paper presentation regarding “Comparison of Respiratory Function in the Prone Maximal Restraint Position With and Without Additional Weight Force on the Back,” I was actually EXCITED to learn of the study, and even HOPEFUL that it would provide important (relevant) information regarding the causes of restraint asphyxia deaths.
However, upon reading Eisele’s paper, I was immediately suspicious of the amount of weight employed for the study. So, the first thing I did after reading it, was to accomplish a personal experience of the study’s methods of weight application while in the PMRP, based upon the descriptions supplied by the study’s authors!
 |
|
1.
“Subject |
|
 |
I scurried around my home looking for common household items that weighed 25 pounds and/or 50 pounds. I couldn’t find a 25-pound household item. So, I decided that I’d rather save time by experiencing the “maximum” weight-force employed for the study, anyway: that of 50 pounds.
DARN! I couldn’t find a 50-pound household item, either. The best I could come up with was a 40-pound, rectangular plastic tub of cat litter (CLEAN cat litter, thank you very much!), and two 5-pound packages of granulated sugar.
After gathering these items, I summoned my mother to assist me. I laid down prone on the cement floor of my basement, reached behind my back, and grabbed my own ankles. Then, I directed my mother to place the 40-pound plastic tub of cat litter on the back of my ribcage, subsequently directing her to place the two 5-pound packages of granulated sugar on top of the litter tub.
This 50 pounds of weight was not at all “comfortable” to support. (The hard edges of the plastic litter tub somewhat painfully dug into the flesh of my back.) But, my BREATHING was not AT ALL perceivably “bothered” by this 50 pounds of weight having been placed on my back, atop my ribcage.
The RIBCAGE is specifically designed to PREVENT compression of the vital organs dwelling within it: the lungs, the heart, and the great blood vessels. Thus, when considering the weight-placement location that Eisele (Chan et al) employed for this study, Eisele (Chan et al)’s study finding “that weight placed on the back during maximal restraint does cause a decrease in spirometry parameters,” was even MORE significant than I had previously recognized.
How much MORE of a “decrease in spirometry parameters” – or OTHER DIMINISHED FUNCTION findings – would have been measured had Eisele (Chan et al) placed even this ludicrously-light amount of weight atop the study subjects’ LOWER BACK; an area NOT supported and protected by a strong bony structure such as the ribcage?!
(4)NEXT; I considered the REAL LIFE “field” situations consistently associated with restraint asphyxia deaths, in relationship to the WEIGHT AMOUNT and WEIGHT-PLACEMENT-LOCATION employed by Eisele (Chan et al) for this study:
In REAL LIFE, if someone is subjected to manually-applied forceful-prone-restraint by one or more adult individuals, at least HALF of one restraining adult individual's weight is applied to the restrained individual's back. (And, that's entirely ignoring the additional "weight" of the "physically-exerted" FORCE applied by the restrainer.)
SO! For “50 pounds” to be considered a “realistic” amount of weight-force application in relationship to FIELD employment of weight to the BACK of a forcefully-prone-restrained person, the restraining individual would have to weigh NO MORE THAN 100 pounds!!!
I don't think I've EVER, in the 15+ years I worked the streets, seen an emergency responder who weighed only 100 pounds. And, certainly, should such a light-weight emergency responder exist somewhere on this planet, she/he would NOT endeavor to restrain an incredibly agitated and violent excited delirium victim ALL BY HER/HIMSELF! Thus, MORE than half the weight of a single 100-pound provider would be applied to the back of any forcefully-prone-restrained individual, because – in a REAL-LIFE forceful-prone-restraint situation – 1 or 2 or 3 or more OTHER (heavier) individuals would be ASSISTING the 100-pounder to restrain the excited delirium victim.
ADDITIONALLY, in REAL LIFE restraint asphyxia cases, there usually is at least ONE person ALSO placing weight on top of the subject’s “lower” back. The lower back is not protected by a rigid, strong, bony structure, such as the ribcage. And, opposite to the lower back is the ABDOMEN.
This means that, weight applied to the area of an individual’s lower back – where there is NO structural protection of a something like a ribcage – immediately causes COMPRESSION of the ABDOMEN … immediately interferes with the DIAPHRAGM’s ability to function … and, thus it IMMEDIATELY INTERFERES with the victim’s ability to BREATHE.
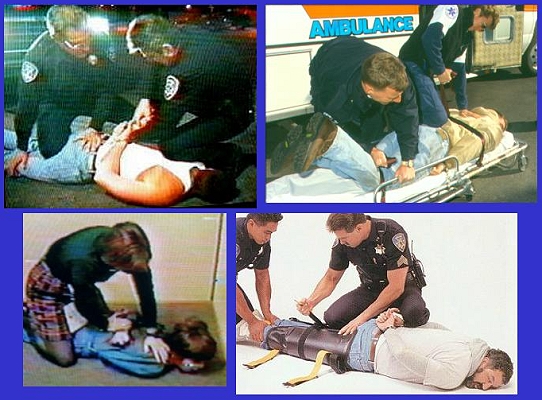
| Were any of the ADULTS being restrained in the posed photos truly a victim of violently-exertive excited delirium, IN REAL LIFE it would take so many restrainers to restrain them, that you wouldn’t be able to SEE the person being restrained!Consequently, there are at least one or two “invisible” restraint participants represented in all but one of the photos at RIGHT.] |
|
 |
It would be a whole helluvalot more HELPFUL if Chan et al would perform a prone restraint “weight study” with their silly little bit of weight (50 pounds) placed on the study subjects’ LOWER BACK. Unfortunately, I don’t believe that Chan et al have ever been honestly motivated to perform a REALISTIC study related to the subject of forceful-prone-restraint and restraint asphyxia. Consequently, I don’t believe that Chan et al would ever be interested in repeating their ridiculous weight study utilizing more realistic study parameters.
(5)LASTLY: NONE of the “weight force during prone restraint and respiratory function” study subjects were EVER required to perform ANY amount of EXERCISE prior to being placed in ANY of the study’s positions, with or without EITHER of the weights applied to their posterior ribcage!
“Each subject was placed into 4 different positions: sitting, PMRP with no weight force, PMRP with 25 lbs of weight force on the back (PMRP_25), and PMRP with 50 lbs of weight force on the back (PMRP_50). Subjects were placed in these positions in random order.Thus, not only were the study subjects entirely HEALTHY and average-weight individuals – not only were they NOT subjected to SOME form of EXERCISE (some form of even MINOR exertion-simulation) prior to assuming a study position – each of them were purposefully given the opportunity to become entirely RESTED prior to being subjected to Chan et al’s 1999 “PMRP” with ridiculously light weights applied to the posterior of their very strong and supportive ribcages.
… Subjects remained in each position for 5 minutes. After each 5-minute period, the subject rested in the sitting position for 10 minutes before starting the next trial.”
It is my opinion that, the failure of this study’s designers to at least subject these individuals to SOME form of EXERCISE (some form of even MINOR exertion-simulation) prior to measuring several of their pulmonary functions while placed in a so-called “Prone Maximal Restraint Position” – with or without silly amounts of weight placed over their RIBCAGE – CLEARLY DEMONSTRATES the fact that these allegedly-professional medical researchers had absolutely NO legitimate interest in performing a study that could yield anything even remotely-resembling MEANINGFUL information.
Each of his “co-authors” allowed him to do so.
Each of his “co-authors” allowed him to do so.
I have not taken the time to determine how many other of Chan’s apparent statements of “fact” made within his spurious discussion of the study findings (or the subject’s research history) are accurately based upon information derived from the references he cites for their support. However, given his track record, it would not at all surpriZe me if there were several other instances of Chan lying about or misrepresenting research articles cited to provide apparent support for his statements – particularly when his statements infer that restraint asphyxia doesn’t happen.
EACH of the study’s authors KNEW THIS when they designed, performed, and subsequently “reported” the 1999 study’s findings.Yet, Theodore Chan was especially motivated to do whatever it took to get this report published. And, each of his “co-authors” allowed him to do so.If ANYONE can provide evidence that ANY of my reveiw comments or conclusions are in any way WRONG or ERRONEOUS, I implore them to SHARE such evidence with me! Unlike Theodore Chan and his ilk, I welcome criticism, and I am happy to amend my conclusions / opinions when provided with “better” information.
Sincerely Yours,
Ms. Charly D. Miller
 Email Charly at: c-d-miller@neb.rr.com
Email Charly at: c-d-miller@neb.rr.com